Examination Date: 2014-03-26
Initial Exam
Chief Complaints
1. Bilateral Lower Back
Below is he findings of the a patient with disc prolapse. He describes a complaint of bilateral lower back pain which began on 2013-10-18. Patient hurt his lower back while twisting the wrong way last year. CT and MR was taken L5-S1 prolapse was noted with mild spinal stenosis. He rated this pain as a 9 on a scale of 0 to 10 with 10 being the worst and considers this condition to be moderate. The pain is constant according to the patient. The pain is described as sharp and stabbing and is radiating into the right buttock, right calf, right foot, right hip and right toes. The pain is reduced by resting while bending, lifting and prolonged sitting aggravates the condition. Additional problems of this condition are numbness, stiffness and tingling.
History
Mr. XXXXXX has recorded that his family doctor is Dr. Tang. The patient denies any surgeries within the past five years. Wrist fracture in 2007 healed now.
Social History
None
Capabilities of Daily Living
The patient states that capabilities of daily living have been affected in the following areas:
Pain restricts lifting only very lightweight objects. I experience SEVERE pain, which reduces my capability to perform any activity. I have CONSTANT pain occurring between 75% and 100% of my awake time.
Physical Examination
Physical examination revealed an individual who was alert, cooperative and orientated.
The patient had a limping gait. The limp appeared on the left.
Sex: Male
Age: 35
Height: 180 cm
Weight: 92 kg
BMI: 28.4
BP: 130/96
Pulse: 86/bpm
Complexion: Normal
Size: Normal
Posture
The patient’s head tilt was to the left. He had a forward head carriage. The patient has rounded shoulders.
Ranges of Motion
Lumbar Spine
Motion Degree Normal Pain Level
Flexion: 11 60 Significant
Extension: 9 25 Significant
Lateral Right: 5 25 Significant
Lateral Left: 5 25 Significant
Neurological Testing
Reflexes Wexler’s Grading System
L R
Patellar (L2, 3, 4) 2+ 2+
Achilles (S1, 2) 2+ 2+
Lower Extremities:
Left Right
L-4 Equal
L-5 Decrease
S-1 Decrease
Lumbar Spine Evaluation
Lumbar spine evaluation provided the following results:
Evaluation of the lumbar spinal region reveals tender areas in the lumbar region on both sides (grade 2) and erector spinae on both sides (grade 2). Palpation of the spine indicated discomfort and pain in the spinous process at: L5 and S1 (grade 3). Evaluation of the lumbar spinal areas indicates that trigger points are present in the erector spinae bilaterally (moderate) and quadratus lumborum bilaterally (moderate). Straight leg raise was positive on the right (14 deg). The patient also reported experiencing radiating pain during the test. Well leg raise was positive on the left (20 deg). Kemps was positive on the left. Kemps was positive on the right. Valsalva’s test was positive. Straight leg raiser test caused pain at 35 to 70 degrees for possible nerve root or disc involvement. This test was followed by Maximal SLR with internal rotation, adduction, foot dorsiflexion, neck flexion and patient bearing down to further pinpoint the lesion. Slump Test in a sited position was also performed to concur with space occupying lesion such as a disc herniation or a bulge. Milgtrams’s (double leg raiser) was also caused radicular pain due to increase of intrathecal pressure. Belt test made no difference during flexion with or without supporting the pelvis. Pain was also felt at hamstrings indicating tightness.
Lower Extremities Muscle Testing
Tibialis 5/5 4/5
Extensor Hallucis Longus 5/5 4/5
Gastrocnemius/Soleus 5/5 4/5
Mr. XXXXXX demonstrated L4 (ankle DF) of 5 lbs on the right and 20 lbs on the left. L5 (big toe extension) of 4 lbs on the right and 8 lbs on the left. S1 (ankle PF) of 8 lbs on the right and 30 lbs on the left.
Diagnosis
M545 Low back pain
S335 Sprain and strain of lumbar spine
M5416 Radiculopathy, lumbar region
Acute, moderate to severe traumatic joint and muscle dysfunction in the above region with associated symptoms of pain, ROM reduction and functional difficulties. This is also consistent with CT and MR findings.
Management Plan
Short Term Goals would be for Mr. XXXXXX to report 50% pain reduction and 50% increase in ROM within 2 weeks. Functionally Mr. XXXXXX should also be able to perform half of his ADL’s within these 2 weeks easier. Long Term Goals would be for Mr. XXXXXX to report over 80% pain reduction and demonstrate over 80% increase in ROM within 4 to 6 weeks. Functionally Mr. XXXXXX should also be able to perform most of his ADL’s within this period. Mr. XXXXXX is also to be discharged with a home exercise program when the above goals have been achieved and he is over 80-90% impairment free.
Spinal Decompression 4-5x per week/duration of 2 weeks.
Therapeutic Exercises 3x per week/duration of 1 month (to improve strength, flexibility, balance, range of motion, or endurance to one or more areas of the body)
Home Exercise Program 1x (for the patient to follow a sound home exercise program to increase flexibility, strength and endurance)
Physical modalities 3x per week/duration of 1 month (Modalities such as heat, cold, electrotherapy, ultrasound, laser, acupuncture and myofascial release are used to reduce pain and inflammation and increase range of motion. )
Today’s Treatments
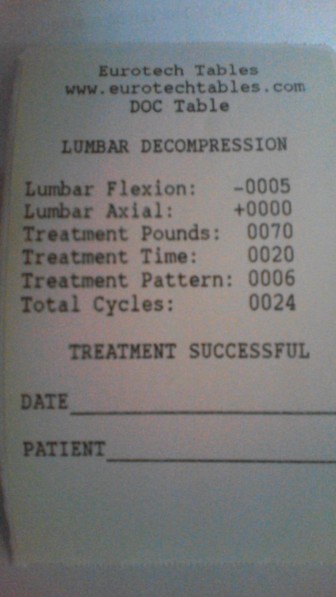
Today’s treatment consisted of interferential (Swing (1-150 Hz 10-20 min)) in the lumbar region; Chiropractic Spinal Decompression (Pron,6,70 lbs,-5deg and20min NP) in the lumbar region.
Prognosis
The prognosis for the patient’s recovery is considered fair.
Notes:
Here is the initial exam and treatment of a new patient that was referred by his medical doctor to us 2 months ago. He did not attend our clinic because he thought his pain will go away. Not only his pain did not go away it actually has become much more severe now; 8-9/10 on VAS. Sometimes discs act like so. The setting of Prone, protocol 6,70 lbs,-5deg for 20 min was initially chose. Electrotherapy was added at the same time to reduce spasm. He was able to get off the DOC table without much pain and no ice was needed.
Also Read
| Case Study: Acute Lumbar Radiculopathy (2) | Case Study: Chronic Lumbar Spinal Stenosis (3) | Case Study: Chronic Lower Back Pain | Case Study: Subacute Lower Back Pain |
| Case Study: Lumbar Spinal Stenosis | Case Study: Right lateral disc protrusion at L5-S1 | Case Study: Antalgic Posture | |